





The Victorian Comprehensive Cancer Centre Alliance (VCCC Alliance) acknowledges that the NLCSP guidelines have been developed in consultation with experts, clinicians, researchers, Aboriginal and Torres Strait Islander peoples, and consumers. We also acknowledge the screening and assessment pathway that outlines the set parameters of the program is based on evidence and expert advice, and that certain program policy parameters are out-of-scope for public consultation, including the program eligibility criteria.
The VCCC Alliance welcomes the opportunity to provide feedback on the proposed eligibility criteria outlined in the draft National Lung Cancer Screening Program (NLSCP) Guidelines. Coordinated by our Program Manager of Aboriginal and Torres Strait Islander Health, this response reflects the VCCC Alliance’s strong commitment to advancing equitable and inclusive healthcare, particularly for Aboriginal and Torres Strait Islander peoples, who experience a disproportionately high burden of lung cancer.
Aboriginal and Torres Strait Islander peoples are a priority population in the program due to inequities in smoking prevalence and access to optimal and culturally safe healthcare, which significantly impacts lung cancer diagnosis, mortality, and survival rates.
Life Expectancy Considerations:
The VCCC Alliance acknowledges the current consultation does not seek feedback on the inclusion criteria for the National Lung Cancer Screening Program (NLSCP). However, we note the opportunity for a formal review in two years and strongly advocate for criteria that reflect the specific needs of Aboriginal and Torres Strait Islander peoples.
This includes consideration about alignment with international best practice around the pack year requirement and lowering the minimum age for screening. The proposed Australian criteria are significantly more restrictive than other nations' screening programs (Refer to Figure 1). We encourage Cancer Australia to prioritise these areas for comprehensive review during the planned evaluation.
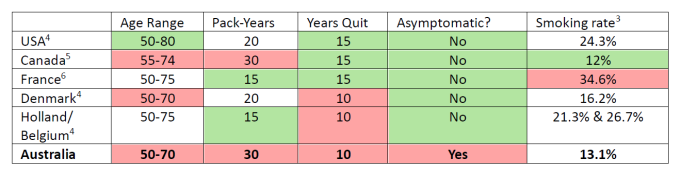
Figure 1: Comparison of the Australian selection criteria with international benchmarks
The VCCC Alliance is committed to collaborating with Cancer Australia and the Victorian State Government to support the program's implementation. This includes exploring innovative models of care to ensure equitable access and effectiveness.
A critical challenge remains in designing systems that adequately support patients and inform the development of culturally safe and patient-centred care models. We look forward to playing an active role in addressing these challenges and ensuring the program delivers optimal outcomes for all Australians, particularly those most at risk.
To ensure the successful implementation of the National Lung Cancer Screening Program and address the unique needs of Aboriginal and Torres Strait Islander peoples, we propose a series of recommendations focused on embedding cultural safety, fostering workforce development, and delivering culturally appropriate care. These measures are essential to building trust, improving access, and achieving equitable health outcomes for Indigenous communities.
Cultural Safety Training and Workforce Development
Mandate comprehensive cultural safety training for ALL program staff, including:
Ensure training is:
Additional Implementation Requirements:
Urgent Mobile Screening Service Priority
While we welcome Heart of Australia's selection as the mobile delivery partner for the NLCSP, we strongly advocate for:
Immediate Multi-State Implementation
Service Implementation Timeline
Operational Requirements
Cultural Safety in Mobile Services
Community Engagement and Integration
Quality Assurance
Given that 90% of lung cancer in Australian men and 65% in women is attributed to tobacco smoking7 and considering the significantly higher smoking rates in Indigenous communities, these modifications are essential for an equitable screening program.
We strongly urge the revision of these guidelines to ensure they adequately serve Aboriginal and Torres Strait Islander peoples. These changes are crucial for closing the gap in health outcomes and addressing the disproportionate burden of lung cancer in Indigenous communities.
1 Australian Government Australian Institute of Health and Welfare. (2018). Cancer in Aboriginal & Torres Strait Islander people of Australia. Retrieved from https://www.aihw.gov.au/reports/cancer/cancer-in-indigenous-australians/contents/cancer-type/lung-cancer-c33-c34
2 Australian Government Australian Institute of Health and Welfare National Indigenous Australians Agency. (2022). Life expectancy at birth. Retrieved from https://www.indigenoushpf.gov.au/measures/1-19-life-expectancy-at-birth#:~:text=The%20life%20expectancy%20for%20First,years%20compared%20with%2083.8%20years)
3 World Population Review. (2024). Smoking Rate by Country 2024. Retrieved from https://worldpopulationreview.com/country-rankings/smoking-rates-by-country
4 U.S. Preventive Task Force. (2021). Lung cancer: screening. Retrieved from https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung-cancer-screening
5 Canadia Task Force on Preventative Health Care. (2016). NEW LUNG CANCER SCREENING GUIDELINE. Retrieved from https://canadiantaskforce.ca/new-lung-cancer-screening-guideline/
6 Pinsky P. F. (2018). Lung cancer screening with low-dose CT: a world-wide view. Translational lung cancer research, 7(3), 234–242. https://doi.org/10.21037/tlcr.2018.05.12
